Early childhood caries
•Download as PPTX, PDF•
20 likes•1,391 views

Early childhood caries (ECC) as the presences of one or more decayed (noncavitated or cavitated), missing (as a result of caries), or filled tooth surface in any primary tooth in a child 71 months of age or younger.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Early childhood caries
Similar to Early childhood caries (20)
More from Alvi Fatima
More from Alvi Fatima (13)
Recently uploaded
Recently uploaded (20)
Early childhood caries
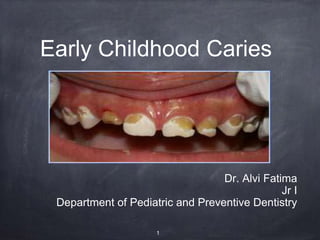
- 1. Early Childhood Caries Dr. Alvi Fatima Jr I Department of Pediatric and Preventive Dentistry 1
- 2. Content Definition of Early childhood caries Terminologies for Early Childhood Caries Classification of Early childhood caries Developmental stages of Early childhood caries Primary etiology risk factor of Early childhood caries Secondary risk factor of Early childhood caries Clinical features Prevention of Early childhood caries Management Barriers in Early childhood caries 2
- 3. Definition The American Academy of Pediatric Dentistry (AAPD) defines Early childhood caries (ECC) as the presences of one or more decayed (noncavitated or cavitated), missing (as a result of caries), or filled tooth surface in any primary tooth in a child 71 months of age or younger. 3
- 4. The AAPD also specifies that, in children younger than 3 years of age, any sign of smooth-surface caries in indicative of sever early childhood caries 4
- 5. Davies (1998)- complex disease involving maxillary primary incisors with in a month of eruption and spreading rapidly to other primary teeth is called childhood caries. Abid Ismail (1998) – early childhood caries is defined as occurrence of any sign of dental caries on the tooth surface during first three years of life. 5
- 6. Terminologies 1) Nursing bottle caries 2) Baby bottle tooth decay 3) Nursing bottle syndrome 4) Milk bottle syndrome 5) Tooth clearing neglect -Moss ( 1996) 6) Infant and Early childhood dental decay – Horowitz 7) Early Childhood Caries –Davies (1998) 8) MDSMD – Maternally Derived Streptococcus Mutans Disease 6
- 7. Classification of Early Childhood caries - by Wayne H 7
- 8. Type I Mild to moderate Existence of isolated caries lesions involving molars and incisors Number of carious teeth increase as cariogenic challenge persists Cause is usually a combination of cariogenic semi solid food and lack of oral hygiene Seen in 2-5 years old 8
- 9. Type II Moderate to severe Labiolingual carious lesion affecting maxillary incisors Mandibular incisors are not affected Use of feeding bottle or at will breast feeding or a combination of both with or without poor oral hygiene Seen soon after eruption of teeth 9
- 10. Type III Severe Carious lesion involve almost all the teeth including mandibular incisors Usually seen in 3-5 years of age Cause is a combination of factors and a poor oral hygiene Rampant in nature and involves immune tooth surface 10
- 12. Stage 1 Clinical stage – Irreversible stage Age – 10-18 months 12
- 13. Features – Cervically and occlusionally interproximal areas of chalky white dimineralization No pain 13
- 14. Stage 2 Clinical Stage - Damaged carious stage Age - 18-24 months 14
- 15. Features – lesion in maxillary anterior teeth, may spread to dentin and show yellowish pain on having cold food items 15
- 16. Stage 3 Clinical stage- deep lesions Age 24-36 months 16
- 17. Features Depending on time of eruption, carogenicity of sweetener and frequency of its use, this stage can be reached in 10 -14 months also Molars are also affected Frequent complaint of pain Pulpal involvement in maxillary incisors 17
- 18. Stage 4 Clinical stage Traumatic stage Age - 36-48 months 18
- 19. Featues – teeth become so weakened by caries that relatively small force can fracture them patient may report a history of trauma molars are now associated with pulpal problems maxillary incisors becomes non vital 19
- 20. 20
- 21. Primary etiology risk factor of Early childhood caries 21
- 22. Dental plaque Mutans streptococci Infant feeding pattern Tooth brushing Salivary factor Sugars Oral clearance of carbohydrates Bovine milk Human milk Fluoride 22
- 23. Secondary risk factor of Early childhood caries 23
- 24. Immunological factor Tooth maturation and defects Race and esthetics Acid fruit drinks Socioeconomic status Dental knowledge Strees 24
- 25. Etiology Bovine milk, milk formulas, and human breast milk have all seen implicated nursing caries because of their lactose content Basic mechanism of demineralization is same and caries tetralogy is key in whole process(microbes, substrates, host, time) Pathogenic microorganism- streptococcus mutans 25
- 26. Steptococcus mutans Main microbe that colonizes teeth after it erupts into oral cavity. It is transmitted to infant’s mouth through mother. It is more virulent because It colonizes the teeth It produces large amount of acid It produces large amount of extracellular polysaccharides that favor plaque formation. 26
- 27. Substrate (fermentable carbohydrate) Carbohydrates are converted into dextrans by microorganisms. 27
- 28. In infants & toddlers, the main sources of fermentable carbohydrates are 1. Bovine milk or infant formulas 2. Human milk (breast-feeding at will) 3. Fruit juices & other sweet liquids 4. Sweet syrups like vitamin preparations 5. Pacifiers dipped in honey or sugar solution 6. Chocolates or other sweets 28
- 29. Host Teeth act as host for microorganisms Hypomineralisation or hypoplasia of teeth increases the susceptibility of child to caries Thin enamel in primary teeth is one of the reasons for early spread of lesions Developmental grooves also may act as plaque retentive areas 29
- 30. Time More the time child sleeps with bottle in the mouth the higher is the risk of caries because the salivary flow and the swallowing reflex decrease. Thus providing more time for accumulation of carbohydrates in the mouth which are acted upon by microbes to produce acid leading to caries. 30
- 31. Other predisposing factors Overindulgences of parents Crowded homes Child who has less sleep Malnutrition Iron deficiency Low birth-weight infants (less than 2500g) 31
- 32. Clinical features A. Maxillary central incisors: facial, lingual, mesial, distal surfaces B. Maxillary lateral incisors: facial, lingual, mesial, distal surfaces C. Maxillary 1st molars: facial, lingual, occlusal, proximal surfaces 32
- 33. Maxillary canines & 2nd molars: facial, lingual, proximal surfaces Mandibular molars: at later stage 33
- 34. Maxillary central incisors: facial, lingual, mesial, distal surfaces 34
- 35. Maxillary canines & 2nd molars: facial, lingual, proximal surfaces 35
- 36. Mandibular anterior teeth are usually spared because of: Protection by tongue Cleansing action of saliva due to presence of the orifice of the duct of sublingual glands very close to lower incisors. 36
- 37. Prevention of Early Childhood Caries • Community based education • Examination and preventive care in dental clinic • Development of appropriate dietary and self care habits at home . 37
- 38. AAPD RECOMENDATIONS FOR PREVENTION OF ECC Infants shouldn't be put to sleep with a bottle . Nocturnal breast feeding should be avoided, parents should be encouraged to have infants drink from a cup Oral hygiene measures should be implemented by the time of eruption of the first primary tooth . An oral health consumption visit is recommended educate the parent and for prevention 38
- 39. RAPIDD SCALE The Readiness Assessment of Parents Concerning Infant Dental Decay (RAPIDD) Scale was developed to/assess a parents stage of change - precontemplative, contemplative or action with regard to his / her child’s dental health . RAPIDD consisted of 38 items with response on five point scale ranging from strongly- agree to strongly disagree 39
- 40. Each of the 38 items were placed in one of the four constructs 1) Openness to health information 2) Valuing dental health 3) Convenience and change difficulty 4) Child permissiveness 40
- 41. PROFESSIONAL AND HOME BASED PREVENTIVE APPROACHES No signs of ECC or low ECC risk status a) Fluoridated dentifrices b) Review of dietary and oral hygiene 41
- 42. Signs of ECC OR high ECC risk status a) Fluoride varnish b) Sealants c) Chlorhexidine varnish d) Xylitol pacifiers e) Fluoridated supplements and dentifrices f) Dietary counseling 42
- 43. MANAGEMENT • Management of existing emergency • Arrest and control of other carious process • Restore and rehabilitation 43
- 44. • Discontinuation of the habit Gradual withdrawal rather than abrupt cessation of the habit Feeding with cup or spoon is encouraged Serial dilution of the contents of the bottle with water Clearance of the milk can be aided by intake of water after feed. Infants must be weaned at 12 to 14 months of age . 44
- 45. Dietary modifications Elimination or gradual reduction of sugar must be done Depending on the child age and chewing capacity natural foods like fruits should be given Oral hygiene measures should be implemented 45
- 46. Factors affecting management • Extent of lesion • Age of the patient • Behavioral problems due to the age of the patient 46
- 47. Treatment can be divided in three visits First visit • All lesions should be excavated and restored • Indirect pulp capping or pulp therapy procedures can be evaluated by further investigation 47
- 48. • If the abscess is present it can be treated by drainage • X-Rays are advised to assess the condition of succedaneous teeth collection of saliva for determining the salivary flow & viscosity • Also, application of fluoride topically 48
- 49. PARENT COUNCELLING Parent should be questioned about the child’s feeding habits, nocturnal bottles, demand for breast-feeding, pacifiers. Parents should be asked to try weaning the child from using the bottle as pacifier while in bed. In case of emotional dependence on the bottle, suggest use of plain or fluoridated water. 49
- 50. The parents should be instructed to clean the child’s teeth after every feed. Parents are advised to maintain a diet record of the child for 1 week that includes the time, amount of food given to the child, the type of the food & the number of sugar exposures. 50
- 51. 2nd VISIT Should be scheduled 1 week after 1st week. Analysis of diet chart & explanation of disease process of child’s teeth 51
- 52. Isolate the sugar factors from diet chart & control sugar exposure Reassess the restoration and redo if needed Caries activity tests can be started & repeated at monthly interval to monitor the success of treatment 52
- 53. 3rd & SUBSEQUENT VISITS • Restoring all grossly decayed teeth Endodontic treatment 53
- 54. In case of unrestorable teeth, extraction followed by space maintainer Crowns given for grossly decayed & endodontically treated teeth Review & recall after every 3 months 54
- 55. Barriers in early childhood caries Lack of involvement and commitment from dental and health organizations. The dental community lacks a shared vison of the definition of the problem , how to prevent it and who is responsible for planning and implementation. 55
- 56. The is no integrated plan to fight the social, economic and nutritional issues facing people in low socioeconomic group. There is weak direct support for research on epidemiology, etiology and prevention of ECC. Dental health is mot a priority of most programs and insurance package. 56
- 57. 57